Received: Tue 19, Sep 2023
Accepted: Fri 06, Oct 2023
Abstract
Background: Among the frequently reported symptoms in long-term COVID-19 syndrome, we can highlight olfactory disorders depression, anxiety, and fatigue. OD can affect people's physical and mental health and can lead to neuropsychiatric symptoms. Objective: Determine the prevalence of symptoms of depression, anxiety, and fatigue in patients with olfactory disorders induced by long-term COVID-19; and investigate this impact on the quality of life. Methods: The study included 30 patients with confirmed long-term COVID-19, with persistent complaints of olfactory dysfunction. OD was evaluated by the connecticut smell test. Neuropsychiatric disorders were evaluated by the fatigue severity and hospital anxiety and depression scales. Quality of life was accessed using the SF-36. Results: 70% of the patients had different degrees of hyposmia and 20% had anosmia. The most prevalent symptom was depression with 66.7% of the sample. More than half of patients also had symptoms of anxiety and fatigue (53,3% both). The most affected dimensions of SF-36 were emotional, vitality, role physical and mental health (36.6 ± 44.0, 44.3 ± 28.7, 47.5 ± 42.7, 49.8 ± 24.7 respectively). There was a moderate negative correlation between symptoms of depression and the physical role and mental health dimension. There was a moderate negative correlation between anxiety and general health, vitality, social functioning, and mental health dimensions. Symptoms of fatigue obtained a moderate negative correlation in the physical function dimension. Conclusion: The prevalence of symptoms of depression, anxiety and fatigue is high in patients with olfactory disorders induced by long-term COVID-19, with a negative impact on the quality of life of these patients, highlighting the role emotional aspect.
Keywords
Long-term sequelae, post-COVID syndrome, neuropsychiatric disorders, olfactory disorders, quality of life
1. Introduction
There are an increasing number of reports of persistent and prolonged effects after the acute phase of COVID-19. This syndrome is characterized by persistent symptoms and/or late or long-term complications beyond four weeks of symptom onset [1, 2]. Some scholars have characterized long-lasting COVID-19 syndrome as symptoms that last more than three months after the onset of the first symptom of the acute phase [3]. This syndrome has been defined by the WHO as a condition that occurs in individuals with a history of probable or confirmed SARS-CoV-2 infection, generally three months after the onset of COVID-19, with symptoms that last at least two months and cannot be explained by an alternative diagnosis [4]. Several meta-analyses investigating the prevalence of post-COVID-19 symptoms have been published, concluding that around 30-50% of subjects who recover from a SARS-CoV-2 infection develop persistent symptoms lasting up to one year [2, 5].
Among the frequently reported symptoms, we can highlight fatigue, with a prevalence of more than 50% in recent studies. Anxiety, depression, and sleep disturbances have been reported in 30-40% of COVID-19 survivors, like survivors of other pathogenic coronaviruses. Fatigue is one of the most described post-COVID-19 symptoms, being reported of 64% in [6] meta-analysis study. Furthermore, age, gender, pre-infection comorbidities (diabetes, asthma) and severity of acute CoV-2 infection (symptomatic/asymptomatic, hospitalization) are confounding factors that could contribute to the development and/or persistence of heterogeneous post-COVID-19 conditions [7].
Another important highlight should be given to chemosensory disorders, including symptoms of olfactory dysfunction (OD) and gustatory dysfunction (GD), which persist or present months after the initial infection. The persistence of OD and GD symptoms after acute COVID-19 is attracting increasing interest and attention from healthcare professionals and the public, as it significantly impacts the quality of life of patients with long COVID-19 [8]. The mechanisms behind the pathophysiology of long-lasting olfactory dysfunction related to COVID-19 is still not known. However, reports of specific brain changes following infection have been observed [9]. A narrative review published in 2023 identified the main risk factors for persistent OD and GD after COVID-19 as being female, the initial severity of the dysfunction, nasal congestion, emotional distress and depression, and variants of SARS-CoV-2 [8].
It is well known that OD can affect people's physical and mental health. Individuals with OD are more likely to suffer from anxiety, depression, and even have a dramatically increased risk of death due to their inability to respond in a timely manner to dangerous odors such as gas leaks, toxic chemicals, and rotting food [9, 10]. Analyzing the impact that neuropsychiatric and chemosensory changes have on the quality of life of patients with long COVID is necessary to guide researchers in the area in directing these patients to specialized treatments. Given this scenario, the main objective of the present study was to determine the prevalence of symptoms of depression, anxiety, and fatigue in a cohort of patients with olfactory disorders resulting from long-lasting COVID-19; and investigate the impact of these symptoms on the quality of life of these patients.
2. Materials and Methods
2.1. Data Sample
A cross-sectional study was performed in a cohort of patients with COVID-19, monitored for late neurological manifestations at University Hospital Gaffree and Guinle, Rio de Janeiro/Brazil from March 2021 to July 2023. Thirty-two consecutive patients with persistent complaints of anosmia/ageusia were invited to participate in the study and evaluated between July 2022 to March 2023. After applying the tests, two patients obtained grades between 6 and 7 in the connecticut smell test, being classified as normosmia. As they did not have smell disorders, these patients were excluded from the study. Each of the thirty remained patient presented a mild form of the disease, without the need for hospitalization or mechanical ventilation, but reported an impaired quality of life due to dysfunctional olfactory ability. COVID-19 was confirmed using a biomolecular assay (RTPCR).
All tests were applied at the same day by 2 researchers. The total time for applying the tests was 25 minutes. This study was conducted in accordance with the ethical guidelines of the Declaration of Helsinki. All patients agreed to participate in the study and signed an informed consent form. The study was approved by ethical review board (protocol number CAAE: 33659620.1.1001.5258).
2.2. Quantification of Impairment of the Olfactory Function
Olfactory functions were evaluated using the connecticut smell test, previously validated to Brazilian Portuguese language [11]. This test assesses both the olfactory threshold (butanol threshold test) and the identification of different odors (identification test), allowing an evaluation both quantitative and qualitative of smell function.
Scores for the butanol threshold test and identification tests were subsequently averaged to arrive at a composite score for olfactory ability, classified as normosmia (score 6-7), mild hyposmia (5-5.75), moderate hyposmia (4-4.75), severe hyposmia (2-3.75) and anosmia (0-1.75).
2.2.1 Butanol Threshold Test
For the olfactory threshold test, we used butanol (n butyl alcohol) diluted at seven different concentrations (4%, 1%, 0.4%, 0.1%, 0.05%, 0.01% and 0.005%). The different concentrations of butanol were placed in amber flasks, with the total solution comprising 60 mL. The flasks were numbered from 1 to 7, from the highest to the lowest concentration. A flask containing odor less distilled water (flask 8) was used as control. The threshold test was performed by presenting the individual with two identical 60 mL flasks alternately, one containing distilled water (flask 8) and the other a butanol solution. With eyes closed, the subjects were instructed to occlude one of the nostrils while the bottle was placed in the non-occluded nostril, asking the subject to inhale gently to identify the presence of the odor. If the individual could not identify the odor, flasks with more concentrated solutions of butanol were presented consecutively, while maintaining the alternation with the flask 8.
The testing was started by exposing the individual to the lowest concentration of butanol (0.005%) until the detection of the flask with the subsequent higher concentration, with retesting being carried out when necessary. Two correct identifications of the flask containing the odorant determined the minimum concentration defined as the individual's olfactory threshold for the tested nasal cavity. The same steps were repeated in the contralateral nasal cavity. The score ranged from 0 to 7 points, with 0 being the individual who was unable to identify the flask containing the odorant at any concentration, and 7 being the individual who identified the odorant in the flask with the lowest concentration.
2.2.2. Identification Test
Eight substances, stored in opaque bottles, were used for the substance identification test: coffee powder, cinnamon powder, talc (Johnson & Johnson® baby powder), paçoca (Paçoquita®), chocolate powder (Nescau®), soap neutral (Palmolive®) and mothballs. With their eyes closed, subjects were instructed to inhale different substances into one nostril at a time. Then, they were instructed to choose from a printed list containing the correct items and the same number of distracting items, the previously inhaled substance. Possible scores ranged from 0 to 7 items correctly identified. Scores from both nostrils were averaged. The final test score was then added to the butanol threshold test for the final result.
2.3. Evaluation of Neuropsychiatric Disorders and Quality of Life
2.3.1. Fatigue Severity Scale
The fatigue severity scale (FSS) consists of nine items that assess the intensity of fatigue and its severity in relation to certain activities in the evaluated patients [12]. The items are scored on a likert scale, where one is “strongly disagree”, and seven is “strongly agree”. The total number of points may vary from nine to 63, with values equal to or greater than 28 indicating fatigue [12, 13].
2.3.2. Hospital Anxiety and Depression Scale
The hospital anxiety and depression scale (HADS) is a self-assessment scale that identifies the presence of anxiety and depression symptoms. It consists of 14 questions, divided into seven subdomains. Scores are based on a four-point likert scale, ranging from zero (never) to three (always). Scores below seven indicate unlikely anxiety/depression, eight to 11 possible anxiety/depression, and scores between 12-21 indicate probable anxiety/depression. Higher scores suggest greater intensity of clinical symptoms. HADS was previously validated for the Brazilian population [14]. Scores equal to or greater than 8 were considered indicative of depression and anxiety.
2.3.3. Medical Outcomes Study 36 - Item Short-Form Health Survey
To access quality of life, the medical outcomes study 36 - item short-form health survey (SF-36) were applied. SF-36 is a widely used scale that evaluates health-related quality of life, and its reliability and validity have been documented in portuguese. It comprises 36 questions which cover eight domains of health. Each domain was scored on a 0-100 metric scale, with a higher score reflecting better health [15]. A mean score of 50 was considered a normative value for all subscales [16].
2.4. Statistical Analysis
Descriptive statistics were obtained for demographic and clinical variables such as age, and gender. The data analysis was performed according to the distribution of the data. The Shapiro Wilk test was used since the sample consisted of less than 50 individuals. Normally distributed variables were plotted as means and standard deviations, and abnormally distributed variables were plotted as medians and interquartile ranges (IQR, defined as the 25th and 75th percentiles). ANOVA test was used to compare the groups of patients divided by the quantification of olfactory loss.
Pearson’s correlation test was used to analyze correlation between SF-36 quality of life domains and scores from anxiety, depression, and fatigue scores. According to Pearson’s coefficient values, correlation was classified as strongly for values ≥ 0.8 positive or negative, moderate if 0.5≥ 0.7 positive or negative, weak 0.2 ≥ 0.4 and 0.0 ≥ 0.2 positive or negative (negligible correlation) [17]. Statistical significance was set at p < 0.05. Statistical analyses were performed using the IBM SPSS statistics for Windows version 22.0; (IBM Corp., Armonk, NY, USA).
3. Results
The median age was 42.0 [33.2- 57.5] years, and none of the patients were older than 68 years. Most of the sample was composed of women (90%) and most had COVID-19 in the year 2020. The clinical and demographic characteristics of the study participants are shown in (Table 1). The median time to maintenance of olfactory and gustatory disorders was 13 [10.8-13.0] months. According to the connecticut olfactory test, 70% of the patients had different degrees of hyposmia and only 20% anosmia (Figure 1). The most prevalent symptom was depression with 66.7% of the sample. In anxiety and fatigue screenings, more than a half of the patients (53,3%) also met the criteria for these symptoms.
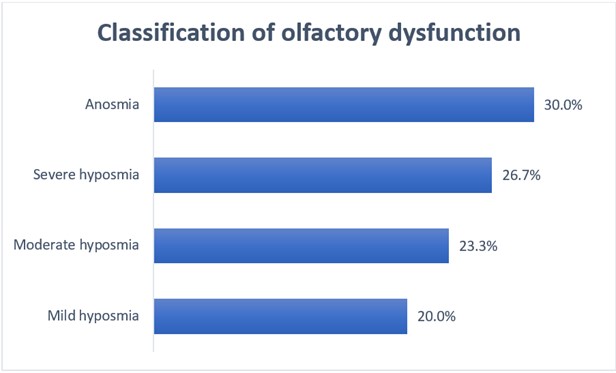
TABLE 1: Clinical and
demographic characteristics of the long-term COVID-19 patients (n=30).
|
Characteristics |
n (%), Median [IQR] or Mean (SD) |
|
Age, Years (median) |
42.0 [33.2- 57.5] |
|
Sex (%) |
|
|
Female |
27 (90.0) |
|
Male
|
03 (10.0) |
|
Year of
COVID-19 infection (%) |
|
|
2020 |
18 (60.0) |
|
2021 |
4 (13.3) |
|
2022 2023 |
6 (20.0) 2 (6.7) |
|
Butanol
score (mean) |
3.0 [1.2 – 4.7] |
|
Fatigue
Raw Score (median) |
29.5 [18.0 – 39.5] |
|
Anxiety
Raw Score (median) |
7.5 [7.0 – 11.7] |
|
Depression
Raw Score (median) |
8.5 [6.0 – 13.0] |
|
SF-36
Subscales (means) |
|
|
77.5
(± 21.2) |
|
|
Role Physical |
47.5 (± 42.7) |
|
Bodily Pain |
65.4 (± 25.8) |
|
General Health |
56.6 (± 23.6) |
|
Vitality |
44.3 (± 28.7) |
|
Social Functioning |
65.4 (± 29.5) |
|
Role Emotional |
36.6 (± 44.0) |
|
Mental Health |
49.8 (± 24.7) |
|
Total |
30 |
IQR: interquartile range;
n: number of patients; SD: standard derivation; SF-36: Expanded version SF-36
short-form 36-item questionnaire.
Regarding quality of life, the most affected dimensions were emotional aspects, vitality, role physical and mental health (36.6 ± 44.0, 44.3 ± 28.7, 47.5 ± 42.7, 49.8 ± 24.7 respectively). The least affected domains were physical function, bodily pain, and social functioning (77.5 ± 21.2, 65.4 ± 25.8, 65.4 ± 29.5 respectively) as shown in (Table 1). After performing the ANOVA test to compare the groups of patients divided by the quantification of olfactory loss, it was not possible to find a statistically significant difference between the groups. Despite this, it can be observed that the emotional role subdomain was affected in all groups of patients. In (Table 2), the dimensions in orange are those in which the patients had the worst quality of life (means less than 50).
TABLE 2: Comparison
of quality of life subdomains according to the severity of olfactory
dysfunction measured by the connecticut smell test.
|
SF-36
subscales mean (SD) |
Anosmia |
Severe
Hyposmia |
Moderate
Hyposmia |
Mild
Hyposmia |
P value |
|
|
Physical
Function |
67.2 (±24.4) |
91.8 (±08.4) |
71.4 (±22.3) |
80.8 (±19.6) |
.082 |
|
|
Role
Physical |
50.0 (±48.4) |
50.0 (±35.3) |
39.3 (±40.4) |
50.0 (±54.8) |
.958 |
|
|
Bodily
Pain |
57.4 (±26.4) |
70.9 (±20.4) |
59.6 (±28.4) |
77.0 (±28.8) |
.445 |
|
|
General
Health |
54.5 (±22.6) |
56.0 (±29.9) |
55.1 (±21.8) |
62.0 (±23.2) |
.944 |
|
|
Vitality |
45.5 (±32.4) |
42.5 (±33.6) |
35.7 (±24.4) |
55.0 (±23.6) |
.703 |
|
|
Social
functioning |
77.7 (±29.8) |
68.7 (±25.0) |
48.2 (±33.4) |
62.5 (±26.2) |
.255 |
|
|
Role
Emotional |
48.1 (±41.2) |
29.1 (±45.2) |
33.3 (±47.1) |
33.3 (±51.6) |
.837 |
|
|
Mental
Health |
52.9 (±26.2) |
45.8 (±22.6) |
44.0 (±26.5) |
57.3 (±26.7) |
.752 |
|
Green signifies better
quality of life (means ≥ 50) and orange signifies a worse quality of life
(means ≤ 49). Expanded version SF-36 short-form 36-item questionnaire. SD:
standard derivation. *p-values refer to ANOVA.
It is worth highlighting the group of patients with moderate hyposmia who obtained an average score below 50 in more than half of the subdomains of the SF-36 quality of life questionnaire, configuring the group of patients with the worst quality of life. Patients with mild hyposmia have a better quality of life when compared to other groups. These results are presented in (Table 2). Correlation analysis was performed between symptoms of depression, anxiety, and fatigue with the dimensions of the SF-36. There was a moderate negative correlation between symptoms of depression and the physical role and mental health dimension.
Regarding anxiety symptoms, there was a moderate negative correlation with general health, vitality, social functioning, and mental health dimensions. Symptoms of fatigue only obtained a moderate negative correlation in the physical function dimension. These results indicate that the greater the prevalence of symptoms of depression, anxiety, and fatigue, the worse the quality of life of patients especially in the dimensions highlighted in green. The correlation analysis between depression, anxiety and fatigue is presented in (Table 3).
TABLE 3: Correlation
between Health-related quality of life (SF-36) versus depression, anxiety, and
fatigue.
|
SF-36
subscales |
Depression |
|
Anxiety |
|
Fatigue |
|
|
|
Pearson
correlation coefficient (r) |
P value |
Pearson
correlation coefficient (r) |
P value |
Pearson
correlation coefficient (r) |
P value |
|
Physical
Function |
-.350 |
.058 |
-.455 |
.012* |
-.511 |
.004* |
|
Role
Physical |
-.536 |
.002* |
-.411 |
.024* |
-.372 |
.043 |
|
Bodily
Pain |
-.448 |
.013* |
-.450 |
.013* |
-.466 |
.009* |
|
General
Health |
-.358 |
.052 |
-.544 |
.002* |
-.481 |
.007* |
|
Vitality |
-.382 |
.037 |
-.584 |
.001* |
-.494 |
.006* |
|
Social
Functioning |
-.385 |
.035 |
-.540 |
.002* |
-.311 |
.094 |
|
Role
Emotional |
-.477 |
.013* |
-.447 |
.013* |
-.436 |
.016* |
|
Mental
Health |
-.610 |
.000* |
-.610 |
,000* |
-.356 |
.053 |
Green signifies a moderate
correlation (0.5≥ 0.7) and orange signifies a weak correlation (0.2 ≥ 0.4).
Expanded version SF-36 short-form 36-item questionnaire. *p-values refer to
Pearson’s correlation Coefficient.
4. Discussion
Our sample was made up of women (90%), which is in line with several studies, where the female sex is considered a risk factor for long COVID [2, 18, 19]. In the systematic review with meta-analysis conducted by [2], of the 16 articles used to analyze sex as a risk factor for the development of long COVID symptoms, in 14 of them, the female sex was associated with greater risk for long COVID. This meta-analysis revealed that female sex was significantly associated with an almost 50% higher risk of long COVID symptoms [2]. Related results were observed by [20], who also reported that female sex was associated with symptoms of long COVID-19, as well as [21], who pointed to female sex as one of the risk factors for long COVID.
The literature points out that women are more vulnerable to developing long COVID than men. The mechanisms behind this increased risk of long-term COVID-19 remain unknown and deserve investigation. Sex hormones and genetic factors have been proposed as underlying mechanisms, which may also explain the higher prevalence of females in post-COVID-19 syndrome [22]. Regarding the quantitative assessment of olfactory function, most patients in our study had different degrees of hyposmia, ranging from mild to severe. The fact that hyposmia is more prevalent than anosmia in patients with long COVID caught our attention. These findings were also found in the study by [18], which used the Sniffin´ Sticks test to quantify olfactory disorders. The study also found a higher prevalence of hyposmia than anosmia (41.9% and 30.2% respectively). The higher prevalence of hyposmia when compared to anosmia (23.2% versus 18.3%) was also found in the study by [23].
The main objective of the present study was to determine the prevalence of symptoms of depression, anxiety, and fatigue in patients with long COVID. The prevalence of these symptoms was high, with depression being the most prevalent (66.7%), followed by symptoms of anxiety and fatigue (53.3% respectively), which shows us that olfactory disorders can be a debilitating condition, generating an impact negative impact on the mental health of these patients. A study conducted by [24] found symptoms of anxiety and depression in 38% of the sample studied. COVID-19 related olfactory dysfunction has been related to mood disturbances [25], and higher likelihood of depression [2].
Several studies point to fatigue as one of the main and most frequent symptoms observed in patients with long COVID-19. In the sample studied, more than 50% of individuals reported fatigue. These findings are also found in several recent studies. In the study conducted by [21], at least 50% of patients with long COVID who reported fatigue also had olfactory disorders. The high prevalence of fatigue (87.5%) was also reported in the study by [26]. In another recent study, fatigue was present in 55.7% of subjects with long COVID and was even significantly higher in females [27].
The secondary objective in our study was to evaluate the impact of neuropsychiatric changes in patients with olfactory disorders on quality of life. Our results indicated that patients with moderate hyposmia had more altered SF-36 subdomains, resulting in a worse overall quality of life when compared to patients with anosmia, who only showed changes in the role emotional subdomain. This domain, in turn, proved to be the most altered in the entire sample studied, demonstrating how the total or partial loss of smell can negatively affect the emotional state of individuals.
Regarding correlation analysis, we found a statistically significant negative correlation between depression, anxiety, and fatigue with several domains of the SF-36, demonstrating that the higher the prevalence of these symptoms, the worse the quality of life of patients with olfactory disorders induced by long COVID. Al Rasheed et al. [28] assessed the impact of COVID-19 on quality of life using both the SF-36 and the FSS to assess persistent fatigue symptoms. They found, like our study, a statistically significant difference for the physical function, role emotional and vitality subdomains, demonstrating changes in the physical and especially mental health of these patients. The FSS scores were negatively correlated with the physical and mental components of the SF-36.
Our findings indicated that olfactory dysfunction induced by long-term COVID-19 negatively impacts certain SF-36 domains of quality of life more than others and this is comparable to findings from previous research. More studies are needed in this area.
4.1. Limitations and Additional Considerations
A limitation of our study was the small sample size. Future studies with larger populations are needed. Here we provide evidence that neuropsychiatric symptoms are frequent in patients with olfactory disorders, with a negative impact on several domains of these patients' quality of life. There is a lack of studies in the literature on effective treatments for the total rehabilitation of olfactory disorders in patients with long Covid. Intervention studies on olfactory disorders are needed. Systematic reviews are also recommended with the aim of investigating the different types of therapeutic interventions that can be used in the olfactory rehabilitation of these patients.
5. Conclusion
The high prevalence of symptoms of depression, anxiety, and fatigue among patients with olfactory disorders induced by long-term COVID-19 demonstrates the need for a more careful look at these patients to refer them to rehabilitation and neuropsychological support programs. Managing these post-COVID-19 symptoms is essential to reduce the negative impact of COVID-19 on the quality of life of these patients.
Consent to Participate
Written informed consent was obtained from all the patients.
Consent for Publication
Written informed consent was obtained from all the patients.
Competing Interests
None.
Acknowledgment
We would like to thank Guilherme H.M. Fenólio and his research team for providing the validated version of the Connecticut olfactory test to Brazil.
Data Availability
The data that support the article's findings are recorded in the medical records of the post-Covid 19 neurological manifestations outpatient clinic (University Hospital Gaffree and Guinle - UNIRIO, Rio de Janeiro, Brazil) and are confidential.
Funding
This study was funded by a research grant from Chagas Filho Foundation for Research Support in the State of Rio de Janeiro (FAPERJ).
Author Contributions
Déborah S. Sales contributed to conceptualization, performed the analysis, and wrote the paper. Mariana B. Hammerle contributed to conceptualization and performed the analysis. Rayanne da S. Souza contributed to conceptualization, data collection and interpretation. Patricia G. Pinheiro, Débora Viana Freitas contributed to interpretation. Ana Carolina F. Herzog, Daniel Lucas de L. S. Santos, Nathalie Souza de Andrade, Nathalia Cardoso dos Santos, Carolina Garcia Nunez Carrijo contributed to data collection Luiz Claudio Thuler contributed to data analysis, interpretation, manuscript editing. Claudia C. F. Vasconcelos contributed to data interpretation, manuscript editing and final approval of the manuscript. All authors contributed to study design and reviewed or edited the manuscript.
REFERENCES
[1] Ani Nalbandian, Kartik Sehgal,
Aakriti Gupta, et al. “Post-acute COVID-19 syndrome.” Nat Med, vol. 27,
no. 4, pp. 601-615, 2021. View at: Publisher Site | PubMed
[2] Kin Israel Notarte, Maria Helena
Santos de Oliveira, Princess Juneire Peligro, et al. “Age, Sex and Previous
Comorbidities as Risk Factors Not Associated with SARS-CoV-2 Infection for Long
COVID-19: A Systematic Review and Meta-Analysis.” J Clin Med, vol. 11,
no. 24, pp. 7314, 2022. View at: Publisher
Site | PubMed
[3] Christin Heidemann, Giselle Sarganas,
Yong Du, et al. “Long-term health consequences among individuals with
SARS-CoV-2 infection compared to individuals without infection: results of the
population-based cohort study CoMoLo Follow-up.” BMC Public Health, vol.
23, no. 1, pp. 1587, 2023. View at: Publisher Site | PubMed
[4] Joan B Soriano, Srinivas Murthy, John
C Marshall, et al. “A clinical case definition of post-COVID-19 condition by a
Delphi consensus.” Lancet Infect Dis, vol. 22, no. 4, pp. e102-e107,
2022. View at: Publisher
Site | PubMed
[5] Qing Han 1, Bang Zheng 2 3 4, Luke
Daines, et al. “Long-Term Sequelae of COVID-19: A Systematic Review and
Meta-Analysis of One-Year Follow-Up Studies on Post-COVID Symptoms.” Pathogens,
vol. 11, no. 2, pp. 269, 2022. View at: Publisher Site | PubMed
[6] Preeti Malik, Karan Patel, Candida
Pinto, et al. “Post‐acute COVID‐19 syndrome (PCS) and health‐related quality of life (HRQoL)-A
systematic review and meta‐analysis.” J Med Virol, vol. 94, no. 1,
pp. 253-262, 2022. View at: Publisher
Site | PubMed
[7] Mikki Jaramillo, Thankam P
Thyvalikakath, George Eckert, et al. “Characteristics of Chemosensory
Perception in Long COVID and COVID Reinfection.” J Clin Med, vol. 12,
no. 10, pp. 3598, 2023. View at: Publisher
Site | PubMed
[8] Bo Lia, Yi-Ke Deng, Ming Zeng, et al.
“Long-term Consequences of COVID-19: Chemosensory Disorders.” Curr Allergy
Asthma Rep, vol. 23, no. 2, pp. 111-119, 2023. View at: Publisher Site | PubMed
[9] Anja L Winter, Sofie Henecke, Johan N
Lundström, et al. “Impairment of quality of life due to COVID-19-induced
long-term olfactory dysfunction.” Front Psychol, vol. 14, pp. 1165911,
2023. View at: Publisher
Site | PubMed
[10] Thomas Hummel, David T Liu, Christian
A Müller, et al. “Olfactory dysfunction: etiology, diagnosis, and treatment.” Dtsch
Arztebl Int, vol. 12, no. 9, pp. 146-154, 2023. View at: Publisher Site | PubMed
[11] Guilherme H M Fenólio, Wilma T
Anselmo-Lima, Gabriela C Tomazini, et al. “Validation of the Connecticut
olfactory test (CCCRC) adapted to Brazil. Braz J Otorhinolaryngol, vol.
88, no. 5, pp. 725-732, 2022. View at: Publisher Site | PubMed
[12] L B Krupp, N G LaRocca, J Muir-Nash,
et al. “The Fatigue Severity Scale.” Arch Neurol, vol. 46, no. 10, pp.
1121-1123, 1989. View at: Publisher
Site | PubMed
[13] M F Mendes, H P Tilbery, S Balsimell,
et al. “Fatigue in multiple sclerosis relapsing-remitting form.” Arq
Neuropsiquiatr, vol. 58, no. 2B, pp. 471-475, 2000. View at: Publisher Site | PubMed
[14] N J Botega, M R Bio, M A Zomignani,
et al. “Mood disorders among inpatients in ambulatory and validation of the
anxiety and depression scale HAD.” Rev Saude Publica, vol. 29, no. 5,
pp. 359-363, 1995. View at: Publisher Site | PubMed
[15] J E Ware Jr, C D Sherbourne “The MOS
36-item short-form health survey (SF-36). I. Conceptual framework and item
selection.” Med Care, vol. 30, no. 6, pp. 473-483, 1992. View at: PubMed
[16] Evangelos C Fradelos, Stylianos
Boutlas, Eleni Tsimitrea, et al. “Perceived Symptoms, Mental Health and Quality
of Life after Hospitalization in COVID-19 Patients.” J Pers Med, vol.
12, no. 5, pp. 728, 2022. View at: Publisher
Site | PubMed
[17] Kelly H Zou, Kemal Tuncali, Stuart G
Silverman “Correlation and simple linear regression.” Radiology, vol.
227, no. 3, pp. 617-622, 2003. View at: Publisher Site | PubMed
[18] David Dylan García-Meléndez, María
Isabel Morales-Casado, Pilar Quintana Castro, et al. “Persistent olfactory
dysfunction in mild COVID-19 patients: A descriptive study of the
characteristics and association with other symptoms.” Med Clin (Barc),
vol. 160, no. 8, pp. 347-351, 2023. View at: Publisher Site | PubMed
[19] Yasser B Hennawi, Raneem A Alahmadi,
Eithar AlOtaibi, et al. “Olfactory and Gustatory Dysfunctions Following
COVID-19 Infection: Factors That Affect Their Duration in Saudi Arabia.” Cureus,
vol. 15, no. 4, pp. e37317, 2023. View at: Publisher Site | PubMed
[20] Giuseppe Maglietta, Francesca
Diodati, Matteo Puntoni, et al. “Prognostic Factors for Post-COVID-19 Syndrome:
A Systematic Review and Meta-Analysis.” J Clin Med, vol. 11, no. 6, pp.
1541, 2022. View at: Publisher
Site | PubMed
[21] Ana B Cazé, Thiago Cerqueira-Silva,
Adriele P Bomfim, et al. “Prevalence and risk factors for long COVID after mild
disease: A cohort study with a symptomatic control group.” J Glob Health,
vol. 13, pp. 06015, 2023. View at: Publisher Site | PubMed
[22] Elisa Gentilotti, Anna Górska,
Adriana Tami, et al. “Clinical phenotypes and quality of life to define
post-COVID-19 syndrome: a cluster analysis of the multinational, prospective
ORCHESTRA cohort.” EClinicalMedicine, vol. 62, pp. 102107, 2023. View
at: Publisher
Site | PubMed
[23] Marcela Martončíková, Pavel Doležal, Kamila Fabianová, et al. “Remote psychophysical testing of
smell in patients with persistent olfactory dysfunction after COVID-19.” Sci Rep, vol. 13, no. 1, pp.
14090, 2023. View at: Publisher
Site | PubMed
[24] Preeti Malik, Karan Patel, Candida
Pinto, et al. “Post‐acute COVID‐19 syndrome (PCS) and health‐related quality of life (HRQoL)-A
systematic review and meta‐analysis.” J Med Virol, vol. 94, no. 1,
pp. 253-262, 2022. View at: Publisher
Site | PubMed
[25] Tania Llana, Marta Mendez, Sara
Garces-Arilla, et al. “Association between olfactory dysfunction and mood
disturbances with objective and subjective cognitive deficits in long-COVID.” Front
Psychol, vol. 14, pp. 1076743, 2023. View at: Publisher Site | PubMed
[26] Laurence Bamps, Jean-Philippe
Armenti, Mirela Bojan, et al. “Long-Term Consequences of COVID-19: A 1-Year
Analysis.” J Clin Med, vol. 12, no. 7, pp. 2673, 2023. View at: Publisher Site | PubMed
[27] Waleed M Alotibi, Zaid Alzeer, Ibrahim F Alfarhan, et al. “The Incidence of Long-Term Fatigue in Patients Who Achieved Remission From COVID-19 at King Abdulaziz Medical City.” Cureus, vol. 15, no. 1, pp. e33869, 2023. View at: Publisher Site | PubMed
[28] Maha M AlRasheed, Sinaa Al-Aqeel, Ghada I Aboheimed, et al. “Quality of Life, Fatigue, and Physical Symptoms Post-COVID-19 Condition: A Cross-Sectional Comparative Study.” Healthcare (Basel), vol. 11, no. 11, pp. 1660, 2023. View at: Publisher Site | PubMed